
Suite 3, Ground Floor, The Gateway,
312 St Kilda Road, Southbank, VIC, 3006
DANCER’S HIP PAIN: Why surgery isn’t a silver bullet

Dancer’s Hip Pain – Why surgery is not a silver bullet
For all those dancers out there, hip pinching, grabbing and pain can be your biggest barrier when you are in class or rehearsals, or, when you are trying to do a retire, développé or grande battement (or anything for that matter!).
Naturally, when you have hip pain that is restricting your dancing ability you will seek help (we hope!). Sometimes, this help, via your doctor or allied health practitioner (physio, osteo,chiro), may lead you on a path to see a surgeon.
Your surgeon may recommend that you need to have a hip arthroscopy to “fix” your pain and your hip. Your MRI result may have said, labral tear, bony issues and chondral damage – these mean dysfunction and pain, right? We are about to challenge that concept….
So to elaborate on what these mean…
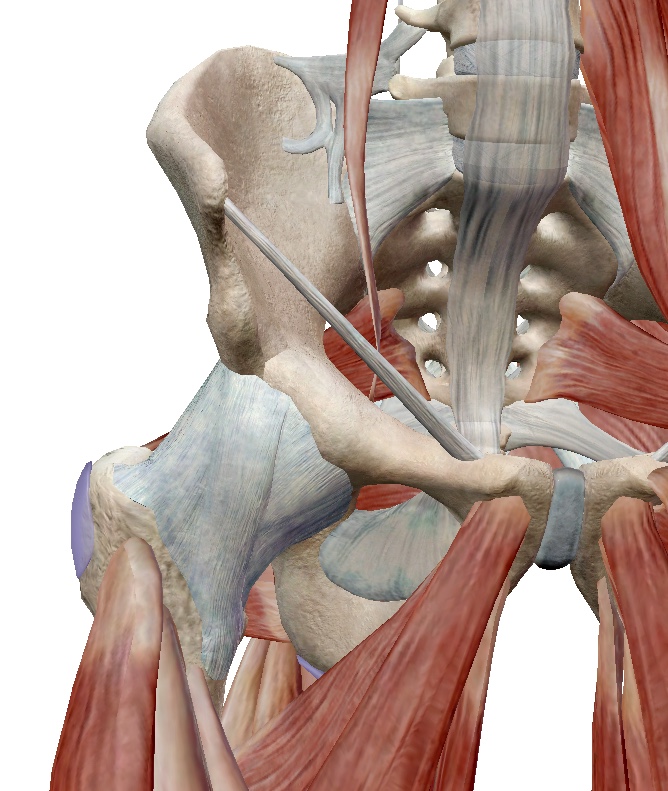
- A labral tear means, a tear in the part of the cartilage in the hip that acts like a suction cup to hold your “ball” in the “socket” (see image)
- Bony issues (or bony morphology) means that shape of your bones (think ball and socket) are creating an issue for you.
- Chondral defects mean that there are issues in the cartilage covering the joint surfaces (think a crack in the lino on the floor).

When you hear such different (and often scary) words, this can be devastating as you don’t know what to expect. However, the surgeon may reassure you that the surgical techniques to either repair or remove the damaged cartilage or offending bone will give you some relief.
Well, interestingly enough…
…The Australian Ballet medical team, have published some of their hip research findings on ballerinas that challenges some of the current ideas and rationale around hip surgery.
The Australian Ballet research has shown that ballet dancers have hip joints that allow them to go into extreme ranges of motion and that dancers’ hips are different from athletes. The research has found that the way your bones are organised (bony morphology) correlates poorly with pain and labral (cartilage) tears. It may mean you are more likely to have issues on the joint surface but overall this is not related to pain. So, to simplify it, this means that if you are a dancer, the way your bones are shaped doesn’t mean you will get a labral tear or pain.
So in summary, in the Australian Ballerinas, cartilage issues and defects in the hip were not related to hip pain. So, if you have an MRI with findings such as “chondral defects” and “labral tear” do not fret. These may not actually be your main issue.
So what are your main issues, I can hear you asking.
Well, the hip is a complex joint with a motion that is rolling, gliding and sliding depending on what movement you are doing and what muscles you are using.
Your issues may be related to muscle activation and patterning.
 If there is an imbalance in how these muscles work then your hip movement may not be as efficient as it could be and you may be feeling discomfort from muscle over activity, fatigue and compression.
If there is an imbalance in how these muscles work then your hip movement may not be as efficient as it could be and you may be feeling discomfort from muscle over activity, fatigue and compression.
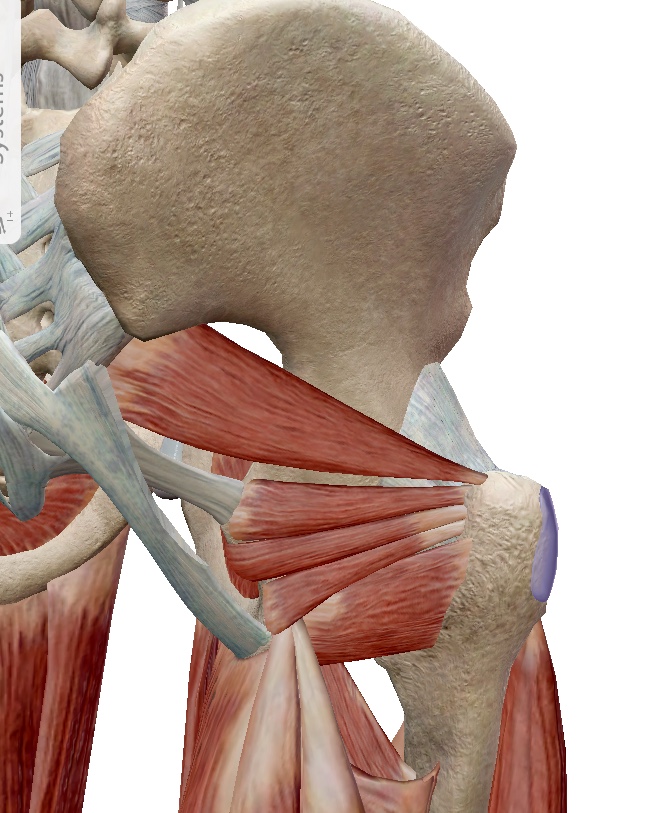
Your hip region has some fantastic deep hip muscles at at the back that act as stabilisers and rotators of the joint (think turn out here). Sometimes, these muscles are not able to activate as well due to an imbalance with the hip flexors, upper gluteal muscles and adductor weakness. This means that your hip joint isn’t going to roll, glide and slide as well as it can, which in turn, feeds your muscular imbalance. So it is a tricky cycle to break.
However, it can be altered with deep focussed exercises to switch on the deeper muscles and switch off the larger muscles so that they can work in harmony together.
(Check out Maddie’s blog on Turn Out to learn about Quadratus Femoris…)
You can then layer exercises over the top to increase adductor and lower gluteus maximus strength (you want to avoid over activity of gluteus medius).
So what should you do?
Having a MRI that seems pretty miserable is not the end of the world. As The Australian Ballet research shows, this may be in the realms of “normal” for you. Seeking guidance from a dance physio or dance doctor is definitely the way to go.
Surgery (and crutches) isn’t necessarily quicker or, in fact, wiser. A focussed treatment and rehab program that is created by physios who understand the ins and outs of ballet and dance is the key here.
Make an informed decision about what is the best treatment for your hip(s) and your body. What do you need your hips to do?
Is it a penché? Is it développé en l’air?
If so, get into the retraining of your hip. It is not always easy but it is a solid base and foundation to hip rehab and decreasing hip pain.
If you want to find out more about your hip, please check out our blogs by Maddie
“TURN OUT“ “CONFESSIONS OF A CRACK ADDICT”
If you are experiencing hip pain and you are a dancer…
Let us help you with treatment and a rehab program that will keep you in the studio and target the real
reason you are getting hip pain.
BOOK ONLINE NOW or CALL US 03 9686 2373
References:
Mayes, S., Smith, P., Cook, J. (2018). Impingement-type bony morphology was related to cartilage defects, but not pain in professional ballet dancers’ hips. Journal of Science and Sports Medicine, 21(9), 905-909
Mayes, S., Ferris, A.R., Smith, P., Garnham, A., Cook, J. (2016). Bony Morphology of the hip in professional ballet dancers compared to athletes. Eur Radiol, 27(7), 3042-4049
Categories :