
Suite 3, Ground Floor, The Gateway,
312 St Kilda Road, Southbank, VIC, 3006
Hip Dysplasia

What is it and how do I gain an accurate diagnosis and treatment plan?
What is Hip Dysplasia?
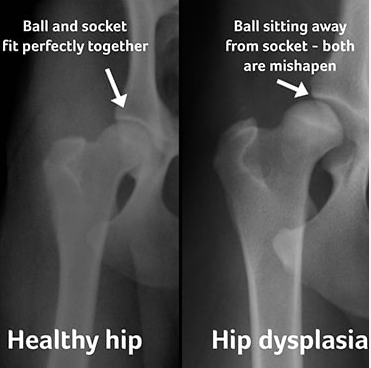
Hip dysplasia covers a range of hip symptoms including pain, instability, and a shallow hip socket. For example, it is generally classified by a loss of conformity between the femoral head (ball) and the acetabulum (socket) of the hip joint. Abnormalities in shape, size, or orientation can cause this.
Clinicians often misdiagnose hip dysplasia, and people can wait on average 5 years and see 3 healthcare providers before receiving a diagnosis. Consequently, it is associated with poorer function, sport & recreation and quality of life outcome measures and has an estimated prevalence of between 3-20% of the population. More severe hip instability and dislocation are more likely to occur during infancy, while a shallow but stable socket is more often diagnosed in adolescence or early adulthood.
What does Hip Dysplasia look like?
Deep hip pain or a limp can be an indicator of hip dysplasia in adolescents and young adults, however this can also indicate other hip disorders. Two or more of the following symptoms increases the likelihood that hip pain may be caused by hip dysplasia.
- History of ongoing deep anterior hip/groin pain (although this could also indicate labral tears, cartilage damage in the joint, or the hip flexor muscles)
- Muscular ache on the side or front of the hip from overworked hip flexor and abductor muscles that are trying to provide more stability to the hip
- Hip pain increases with walking, standing or running
- Pain at night
- A sensation of catching, snapping, popping, or locking that is usually painful
What are the risk factors for Hip Dysplasia?
- Neonates with hip dysplasia: 75% Females
- 80% of people presenting for treatment of Hip Dysplasia are women
- Hypermobility
- Swaddling
- Primiparity & multiple births
- Breech
- Rural childbirth
- Early hospital discharge
- Hereditary/Genetics
- Left Hip 64% (when unilateral)
What is the treatment options ?
Doctors manage hip dysplasia both surgically and non-surgically, but they usually attempt non-surgical management first. Treatment can be dependent on the type of dysplasia, and the age of diagnosis.
Non-surgical treatment:
- Education & advice including reducing aggravating loads, specific lifestyle and exercises modifications.
- Targeted strengthening program: Sway correction, hip abductors, ER, IR strengthening, gym programming, standing stability progressions, multiplanar progressions, single leg work
- Movement pattern retraining
- In babies and infants treatment usually consists of long periods of bracing to help the hip develop in a more stable and aligned position (Pavlik harness) or surgery to realign the joint (open or closed reduction depending on age, spica cast)
In more severe cases of hip dysplasia, where non surgical management has failed or when the hip is very unstable (subluxation/dislocation) surgical intervention may be appropriate. An orthopedic surgeon will determine the treatment plan in these cases.
Surgical treatment:
- Arthroscopy
- Periacetabular osteotomy (PAO)
- Total Hip Replacement (THR)
Hip Dysplasia Summary:
- Misdiagnosis is common as hip dysplasia often masks as FAI (femoroacetabular impingement), hip flexor pathology, GTPS (lateral hip pain), or groin pathology
- Different types of hip dysplasia exist with unique presentations – there is no single rule in/out test and each type is treated differently so it is important to get an accurate diagnosis. This is where weight bearing x-rays are indicated for gold standard diagnosis.
- Non-surgical management should be attempted prior to surgical treatment
- Treatment should be targeted to:
- type of dysplasia
- physical impairments
- functional/athletic demands
- Additionally, education and activity modification play an important role.
- Moreover, graduated, milestone-driven, high-level rehab is crucial prior to return to full function and sport
This is why a thorough assessment and correct referral for imaging or orthopedic intervention is crucial for the optimal management of hip dysplasia. Physiotherapy can help with this and can establish a specific rehabilitation program to reduce symptoms associated with hip dysplasia.
~ Elise McMahon
Categories :